Welcome — use the links above to navigate to different report sections. Get quick takeaways in the Executive Summary. And don’t miss the related resources at the bottom of this page!
As the Thrive Rural Framework makes clear, rural health and rural community and economic development are inextricably connected—neither field can be successful without the other. Thriving economies and communities require healthy people, and people need strong economic and health systems to thrive. Ideally, both fields are aligned and working together toward a common outcome: healthy places where each and every person belongs, lives with dignity, and thrives.
In practice, however, it is all too common for stakeholders from health and rural development to work in silos, talk past each other, or even work against each other as they seek to implement their respective projects—mainly because their funding sources and operating structures do not encourage or reward collaboration across fields. Economic development projects may not consider the impact of industries on community health, for example. Health-focused projects may encourage target populations to adopt practices that aren’t feasible given economic conditions or simply respond to negative outcomes rather than the systemic root cause.
In many cases, traditional approaches to rural development and health aren’t working or equitable. For example, reliance on attracting or retaining a single major employer or industry leaves rural communities vulnerable to boom-and-bust cycles, and one-size-fits-all health promotion programs may not have the desired impact in rural communities and Native nations with their own robust cultures and values.
The pandemic brought the realization that mental and physical health is critical to ensuring you have a thriving workforce. There is broader recognition that you need to ensure that employees have a good quality of life—and when they don’t, their work performance falls off.
Nathan Ohle, CEO, IEDC, Washington, DC
The rural health and development fields can work together to exchange learnings and adopt new approaches from each other. For example, economic development approaches often seek to attract “talent” from other places to build local workforces and entrepreneurial ecosystems rather than bringing people living in rural communities into local economies. Public health approaches, which focus on local populations, could help inform and enrich economic development in such cases—especially in seeing and understanding non-traditional assets/capitals that traditional economic development might miss.
The last few years have brought new resources to rural places to combat the pandemic and improve economic outcomes. With these investments and renewed attention on rural development, we can do rural development and rural health differently—moving collectively toward equitable rural development with projects grounded in place and a people-centered vision of community impact.
If people don’t have access to choose healthy foods, then how do we make nutrition education work for our communities? When they don’t have access to electricity, to running water, to grocery stores? People need the economic opportunities that allow them to buy foods like kale and blueberries.
Denee Bex, Founder and Owner, Tumbleweed Nutrition LLC, New Mexico
To achieve this, we must align mindsets across fields to truly work together toward our common goal. This Call to Action results from thoughtful reflection and engaging conversation among health and rural development practitioners based in rural communities and Native nations across the United States. As these practitioners came together to discuss perspectives and concerns, they laughed together, cried together, and advanced the vital work of aligning mindsets for the sake of rural communities.
This Call to Action is part of a series that aims to equip local- and systems-level actors with equity-centered principles that will lead to equitable, healthy, and long-lasting regional economies in rural communities and Native nations across the United States.
What does success look like?
Exciting ideas for advancing collaborative, equity-focused health and economic development work emerged across the TRALE conversations. Participants were eager to envision how economic development projects could advance health and how health initiatives could advance economic development—grounded in a vision of rural communities and Native nations as healthy places where each and every person belongs, lives with dignity, and thrives.
With successful alignment between rural health and development, participants thought communities could:
Make rural areas places where young people can build thriving careers and start families.
Design our communities and resources so it’s possible for older retirees to age in place.
Build accessible communal spaces—physical infrastructure, green spaces, and spaces for social connection.
Invest in quality and sustainable care systems and care workers (prenatal, parent, child, school, aging, etc.) across the lifespan.
Make systems accessible across barriers, from language to internet access.
Create equitable healthcare institutions with strong antiracism and anti-bias programs.
Develop and fund grow-your-own workforce initiatives, including training more healthcare providers who reflect local communities.
Provide access to clean water, food, and environment. Invest in locally and regionally grown food and distribution.
Restore ownership so that Native folks own the land and prosper on it with their own traditions.
Meet the basic needs of human beings.
It’s smart to think about what you mean by equitable prosperity. Because in the outside world, they’re thinking money. They’re thinking infrastructure. They’re thinking—I want a building, I want a business, and the bottom line is money. When you’re talking about the Native community, and you’re talking about equality—we don’t have our own land, we can’t develop on our land. We have no infrastructure. There’s this white perspective, and there is this Native perspective. We want infrastructure on Navajo. But what does that look like? We do not want to have Phoenix on the reservation. That’s not infrastructure for us. Infrastructure will be water rights, land rights. And that’s what we’re talking about—if we can fix that at its root.
Valerie Tsosie, Founder and President, So’ Tsoh Foundation, Arizona
Definitions
The definitions below are terms and concepts used regularly in this Call to Action.
These definitions should not be considered exhaustive or final but act as a baseline for readers to understand the issues discussed in this document.
Capacity building: developing the ongoing ability of an organization or community to accomplish the goals they set for themselves.
Community conditions: aspects of a community’s circumstances that affect its ability to grow and thrive (e.g., infrastructure, access to resources, environmental status). See also “social determinants of health,” below.
Equity: fairness and justice in outcomes and impact.
Equitable development: development activities undertaken with a focus on fair and just outcomes and processes, especially for communities and people affected by historical and ongoing structural discrimination.
Equitable rural prosperity: the ultimate outcome of the Thrive Rural Framework — communities and Native nations across the rural United States are healthy places where each and every person belongs, lives with dignity, and thrives.
Health equity: everyone has a fair and just opportunity to be as healthy as possible. This requires removing obstacles to health, such as poverty, discrimination, and their consequences, including powerlessness and lack of access to good jobs with fair pay, quality education and housing, safe environments, and health care. (Robert Wood Johnson Foundation)
Racial equity: a process of eliminating racial disparities and improving outcomes for everyone. It is the intentional and continual practice of changing policies, practices, systems, and structures by prioritizing measurable change in the lives of people of color (Race Forward).
Racial justice: a vision and transformation of society to eliminate racial hierarchies and advance collective liberation, where Black, Indigenous, Latinx, Asian Americans, Native Hawaiians, and Pacific Islanders, in particular, have the dignity, resources, power, and self-determination to fully thrive (Race Forward).
Region: an area involving multiple jurisdictions (e.g., counties, states) across which collaborative projects make sense for geographic, cultural, or other reasons.
Rural: Many definitions of rural exist across the health and development fields. Most definitions focus on what rural communities are not—part of large cities or suburbs. Given regional variations in culture and geography, creating an authentic definition of rural that works for all communities is difficult, so self-definition is often the clearest way forward. For this work, Aspen CSG has focused on self-identified rural communities affected by disinvestment and injustice across race, place, and class. For an in-depth discussion of the impact of rural definitions, see Defining Rural America: The Consequences of How We Count, from the Center on Rural Innovation.
Social Determinants of Health: The social determinants of health (SDH) are the non-medical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life. These forces and systems include economic policies and systems, development agendas, social norms, social policies and political systems (World Health Organization). See also “community conditions,” above.
Structural racism: Structural racism refers to the formal and informal discriminatory practices that have occurred historically within institutions, governmental policies and laws, social structures, and culture, as well as those still occurring today. These inequities are deeply rooted and embedded in our social, economic, political, and legal systems.
Sustainability: the degree to which an economic activity is both durable, avoiding boom and bust cycles, and equitable, strengthening and preserving the diverse assets essential to the long-term health of rural communities.
Vital conditions: properties of places and institutions that all people need for health and well-being. They include a thriving natural world, basic needs for health and safety, humane housing, meaningful work and wealth, lifelong learning, reliable transportation, and, central to all of these, belonging and civic muscle (ReThink Health).
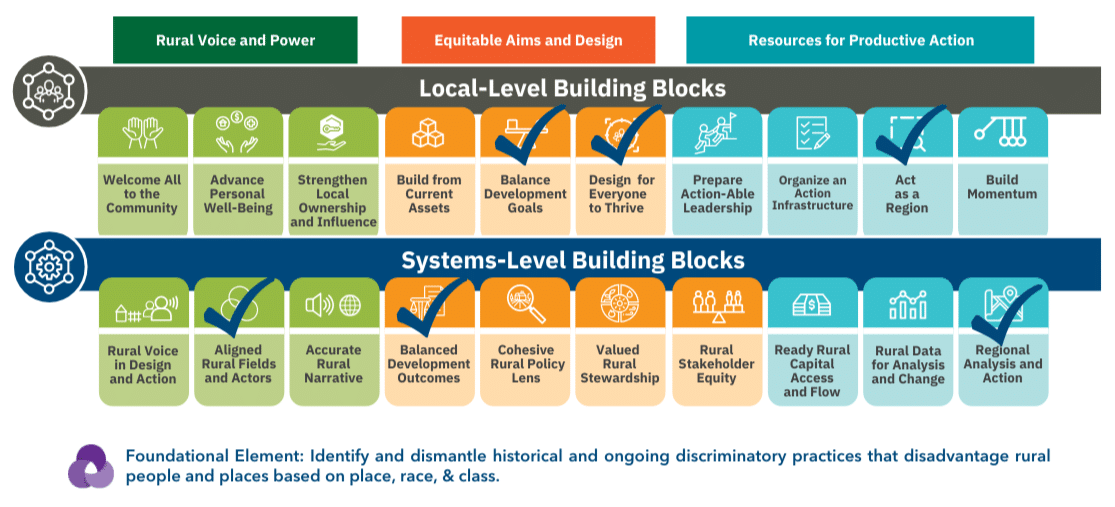
THRIVE RURAL FRAMEWORK BUILDING BLOCKS HIGHLIGHTED IN THIS REPORT
This Call to Action is part of Thrive Rural, which imagines a future where communities and Native nations across the rural United States are healthy places where each and every person belongs, lives with dignity, and thrives. The Thrive Rural Framework provides a shared vision and a line of sight for Aspen CSG’s current understanding of the local and systems conditions necessary to realize that vision.
The TRALE Process: Structure & Participants
This Call to Action results from Aspen CSG’s Thrive Rural Action-Learning Exchange (TRALE). TRALE is a process that quickly taps on-the-ground insights and experiences to help generate breakthrough thinking about what works and what’s needed to push forward policy and practice that improve equitable outcomes for rural communities of color and concentrated poverty.
For this TRALE process, Aspen CSG convened 29 economic and community development practitioners from rural and Indigenous communities across the United States. These rural practitioners, advocates, and innovators shared their experiences and ideas to answer the question, “What will it take to align mindsets so that stakeholders in rural development and health hold a shared understanding of what constitutes ‘equitable prosperity’ in rural regions and Native nations and collectively drive policy, practice, and resources towards producing those results?”
Collectively, the diverse participants account for a high level of experience and expertise in community development, disability justice, economic development, education, environmental justice, health care, philanthropy, public health, racial justice, and wellbeing. They are respected, committed leaders in their communities, representing many regions of the United States, from the Pacific Islands to the Southeast. A detailed list of TRALE participants is provided at the end of this webpage.
Principle #1: Recognize the interconnected goals of rural health equity and rural development and work to align these fields through a common language and shared, overlapping measures of success.
Across our TRALE conversations, the need to develop a shared language and understanding was a consistent theme. For example, a shared understanding of success and community wellbeing does not exist across federal agencies that work in rural communities (these include USDA, EDA, DoE, EPA, HHS, DoH, HUD, and more), nor is this true at state agencies or local county departments.
Many participants noted that people from different contexts use the same words in different ways (e.g., community, development, equity, health), which can get in the way of effectively working together. This has been confirmed by Aspen CSG’s discussions with federal agency staff that there is no shared language or agreement across agencies regarding rural work. To work together toward a shared aim, we need a shared understanding of what that aim means in practice. This may require expanding economic development and health definitions to encompass a more holistic, place-based vision of thriving, equitable communities. It will also require a careful and respectful exploration of where health and rural development work align, overlap, and perhaps conflict. For example, medical providers are often anchor employers and economic engines in rural communities, and leaders of those institutions need to acknowledge their dual roles in both health and development. An excellent example of a resource guiding this work on the local/regional level is the Building Healthy Places, A Playbook for New Rural Healthcare Partnership Models of Investment.
TRALE participants emphasized that developing shared language and aims requires deep listening and building trust, including in contexts where power imbalances have made trust challenging in the past. There is a deep history of exploitation and mistreatment by health service entities with communities of color, just as there is a long history of exclusion, redlining, and predatory practices in economic development efforts. Participants also noted that in developing shared goals and measures of success, it’s essential to consider the causes and conditions that have led to the current state of rural communities and to design solutions commensurate with the histories and challenges involved. (For a deeper analysis of this issue and recommendations about measuring equity reduction, collaboration, and relative change, see Aspen CSG’s Measure Up: A Call to Action, the result of an earlier TRALE process.)
“We have a language barrier between rural health and rural development. We need to adopt shared language, increase respect and openness to practices of both sectors, and collectively shift away from the “we know best” mindset if we truly want to be impactful.”
Shauneequa Owusu, Chief Strategy Officer, ChangeLab Solutions, California
“I think we need to be upfront about where there may be some differences of interests. For example, in some small communities, a nursing home may be the major employer, and the interests of nursing home operators don’t always align with the needs of the community—especially people with disabilities in those communities who want to live independently. And so I think we need to acknowledge that and figure out ways to make it work so that there is economic development—but the kind of economic development that empowers all the residents.”
Dan Kessler, Association of Programs for Rural Independent Living (APRIL), Alabama
“We need to expand the definition of economic development and recognize the significance of place. Within that expanded definition, we would ensure that economic development activities would always be connected to social outcomes, and encourage cross-sector collaboration as we build rural communities from the bottom up. We would have intentional processes for ordinary people to educate lawmakers and philanthropic organizations and speak on their own. We would not just have representatives of interest groups speaking for local people. We would not just provide technical assistance for grant writing, but we would be intentional in creating opportunities for rural people to understand the process itself and how it actually works. We would rethink how philanthropy funds communities and ask that capacity building resources, and sustainability resources be included in philanthropic processes.”
Veronica Lee Womack, Executive Director, Georgia College and State University’s Rural Studies Institute, Georgia
Aligning in polarized times
Finding shared language can be especially challenging in our current politically polarized landscape, where some words like “equity” have taken on meanings associated with political identities. TRALE participants noted that using plain language and sharing stories can help make connections across divides, but there is a risk of reinforcing inequitable systems if you can’t speak about them directly. (For more on this issue and how one dynamic organization addresses it, see Aspen CSG’s Case Study Communicating for Connection: West Virginia Community Development Hub.)
Principle #2: Align funding, planning, implementation, and evaluation systems across the rural health equity and rural development fields to advance common goals.
Even when actors within the rural health and development fields use the same language and work toward the same goals, the systems and structures associated with the two fields work separately, often repetitively, and sometimes at odds. For example, both rural health and economic development systems require specific planning and assessment processes within each community (e.g., Community Health Needs Assessment (CHNA), Comprehensive Economic Development Strategy (CEDS)). Planning and assessment processes in both fields require extensive community input and data gathering, and the same community members are often called upon to contribute to both. Parallel processes also happen across the project lifespan, from funding (grants with similar aims but very different timing and requirements) to implementation (projects working toward similar goals without active collaboration) and evaluation (measuring similar indicators multiple times). Collaboration and coordination across agencies and fields could allow these processes to become complementary rather than parallel or conflicting, enabling communities to better meet their goals. A key aspect of this work will be an acknowledgment across fields of the significance of place: all plans and processes should center and serve the place, rather than the reverse.
“Part of the problem of bringing health and wealth determinants together is that it can be challenging from a strategy perspective—this has been a sticking point.”
Victoria Faust, Senior Learning & Evaluation Officer, Colorado Health Foundation, Colorado
Funding is always a throughline in discussions about equitable rural development. TRALE participants agreed that funding mechanisms need to shift in specific ways to accommodate shared definitions and goals. For example, broadening definitions of economic development or health promotion could allow for projects more likely to get to the root causes that prevent communities from experiencing equitable development. Funding agencies also have the power to require grantees to report on metrics around integration and collaboration between fields, and this could have a unifying field impact if implemented thoughtfully.
“Perhaps we can coalesce a multidimensional space of support that isn’t relying on just philanthropy, the government, or any private company. No entity alone can solve the myriad of challenges in rural communities. We’ve got to be in this together.”
Lisa Medellin, Director of Programs, Healthcare Georgia Foundation, Georgia
Principle #3: Bring together resources across rural health equity and rural development to design and implement projects grounded in community assets, awareness of exclusionary histories, and leadership of those most affected.
TRALE participants were very clear that one key to aligning work across fields toward equitable rural development is to keep the work focused on—and led by—Black, Indigenous, Latino, Asian, and low-wealth rural people and communities at all levels. Practitioners across the country have experienced the disconnects and harm that can occur when outside actors—funders, government agencies, or national organizations—attempt to work on rural and Indigenous people and communities rather than partnering with them. This applies to both health and community development efforts and their alignment, and it requires strong and equitable partnerships between government, philanthropy, practitioners, and communities.
Keeping people at the center and communities in the lead when addressing development and health issues will require interrupting traditional power dynamics related to race, place, and class—within rural communities and between rural communities and outside actors. This means considering and welcoming the full participation of all people in the community, not just considering them as a means to an end in terms of demonstrated outreach or approval of already-developed plans. It also means engaging with and adapting to local culture and building trusting relationships within and across communities in the region.
“There’s a need for the right kind of support and technical assistance for groups in rural communities—folks that actually understand specific context, dynamics, and realities in rural communities who can provide a range of technical services. I think it’s deeper than hiring a grant writer or a someone with a cookie-cutter approach – you need someone who understands the kinds of barriers or challenges a group is facing in their community, what kind of change they’re trying to drive, and how that work can be translated to other funders and partners to foster connection, understanding, and a more collaborative relationship.
K. Jehan Benton-Clark, Principal, IMPACT Practice Advisors, Georgia
Investing in local capacity is also a vital element of this principle—this includes both the inclusion and development of local leaders and investment in community organizations that are trusted connectors and hubs in the region. This ensures communities can partner on equal terms with health and rural development practitioners to build on the assets and strengths that they have. TRALE participants also emphasized that shifting reporting requirements and administrative burdens around funding opportunities could allow these community-based organizations to take on projects responsive to local conditions.Grounding work locally and regionally through Rural Development Hubs is an essential strategy for alignment and accountability. These hubs can be a source of expertise and assistance for communities and an intermediary to help translate between communities and outside organizations.
Rural Development Hubs
Rural Development Hubs are the main players in rural America that are doing development differently. Hubs think of their job as identifying and connecting community assets to market demand to build lasting livelihoods, always including marginalized people, places, and firms in both the action and the benefits. They focus on all the critical ingredients that either expand or impede prosperity in a region—the people, the businesses, the local institutions and partnerships, and the range of natural, built, cultural, intellectual, social, political, and financial resources. They work to strengthen these critical components and weave them into a system that advances enduring prosperity for all.
Hubs play a transformative role in their regions and communities. They are not focused on meeting immediate needs alone. They also aim for and deploy systemic and long-term interventions and investments to strengthen the essential components that form a better foundation for lasting prosperity.
“We need to start to define ourselves as rural development hubs and become recognized as that. To develop the whole Thrive Framework, instead of giving funds to state or national organizations to come into an area where they don’t have boots on the ground, fund the hub itself.”
Nancy Van Milligen, President and CEO, Community Foundation of Greater Dubuque, Iowa
List of TRALE Participants
Calvin Allen, Vice President for Partnerships and Programs, MDC, North Carolina
Marie Barry, Director of Community Economic Development, Rural Wisconsin Health Cooperative, Wisconsin
Jehan Benton-Clark, Principal, IMPACT Practice Advisors, Georgia
Jennifer Bevis, Senior Rural Advocate, Blandin Foundation, Minnesota
Denee Bex, Founder and Owner, Tumbleweed Nutrition LLC, New Mexico
Grace Blanchard, Program Manager, National Association of Counties, Washington, DC
Jessa Chabeau, Regional Manager, Appalachia, Environmental Health Project, Pennsylvania
Ernestor De La Rosa, Regional Manager, Local Government and Community Affairs, ITC Holdings Corp., Kansas
Barb Fabre, CEO, Indigenous Visioning, Minnesota
Victoria Faust, Senior Learning & Evaluation Officer, Colorado Health Foundation, Colorado
Kiersten Frobom, Senior Analyst, County Health Rankings and Roadmaps, University of Wisconsin, Population Health Institute, Wisconsin
Dr. Laura Gerald, President, Kate B Reynold Charitable Trust, North Carolina
Sabrina Golling, Program Manager, Rural Forward, MDC, North Carolina
Lee-Ann Heely, Director, Hawai’i Island Community Health Center, Hawaii
Dan Kessler, Association of Programs for Rural Independent Living (APRIL), Alabama
Charley Martin-Berry, Director, Community Caring Collaborative, Maine
Lisa Medellin, Director of Programs, Healthcare Georgia Foundation, Georgia
Nancy Molina, Colorado Department of Public Health and Environment, Colorado
Amanda North, Center for Rural Health Innovation, North Carolina
Nathan Ohle, CEO, IEDC, Washington, DC
Shauneequa Owusu, Chief Strategy Officer, ChangeLab Solutions, California
Anna Rondon, Project Director, New Mexico Justice and Equity Institute, New Mexico
Tim Size, Executive Director, Rural Wisconsin Health Cooperative, Wisconsin
Tipiziwin Tolman, Adjunct Faculty, Washington State University, Washington
Paula Tran, State Health Officer and Division of Public Health Administrator, Wisconsin
Department of Health Services, Wisconsin
Valerie Tsosie, Founder and President, So’ Tsoh Foundation, Arizona
Nancy Van Milligen, President and CEO, Community Foundation of Greater Dubuque, Iowa
Mary Willard, Director of Training and Technical Assistance, Association of Programs for Rural Independent Living (APRIL), Montana
Veronica Womack, Executive Director, Georgia College and State University’s Rural Studies Institute, Georgia
Support for this report was provided by the Robert Wood Johnson Foundation. The views expressed here do not necessarily reflect the views of the Foundation.
Aspen CSG’s consultant, Rebecca Huenink, led the writing process for this report. We are grateful for her contributions.